The Style Template editor allows for changing the background and text color of the page and the sections below, as well as inserting links, images, and styled Lists. However, Bold, Italic,..., xl, xxL etc. do not have the UNDO function. However, instead of undo, you can highlight the text, cut, paste as unformatted text and redo the styling
For more involved editing, use a word processor or wysiwyg html editor. Style and design as you like; copy from the editor and paste the content into any editable section of this document.
Images can't be copied from editors. Insert them separately
Page Areas
Choose the font family for this page.
Choose text-color for the areas below:
Lists Examples: copy, paste, and overwrite
apples
bananas
apples
bananas
Parkour n.
The art of running and jumping while navigating obstacles
Football n.
The art of running and jumping while navigating people.
make a hyperlink
copy and paste the link
make imagenote
type image location in URL
•default is image right, text left
•click checkbox for image left
click on
•resize the image as desired with the range bar
copy the image
•first select the image (image will highlight)
•in Firefox double click to select
•in Chrome click as if to grab, then drag and let go. Image will be selected
Copy the image (¡;normal!)
•do not "copy image" from right-click (it will lose it's resize)
•use right-click "copy" or ctl+c
close or
•so you can see the page again
Paste image in desired place
If you don't like the size or alignment...
•select and delete the image
•make image again, copy, paste
setzztopz
19
[ ... Edit Mode ... ]
Ctl + z [undo] Ctl + y [redo]
Arrhythmia Cheat Sheet
Title
Article
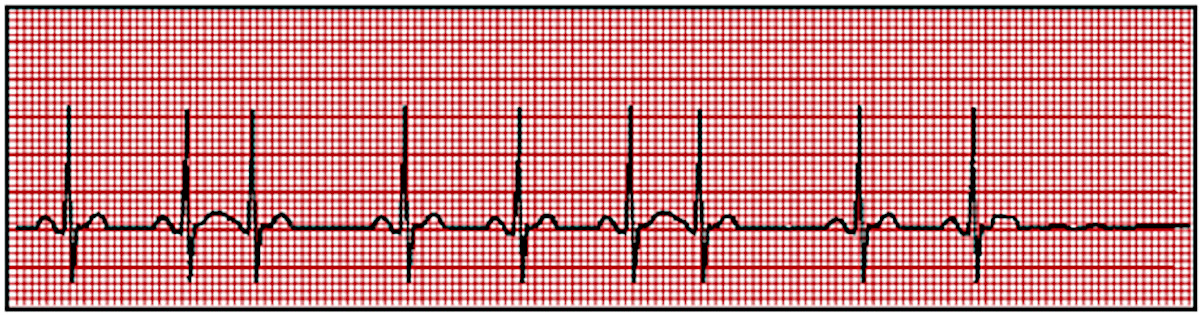
Sinus Arrhythmia
Irregular atrial and ventricular rhythms. Normal P wave preceding each QRS complex.
Normal variation of normal sinus rhythm in athletes, children, and the elderly. Can be seen in digoxin toxicity and inferior wall MI.
Atropine if rate decreases below 40 bpm.
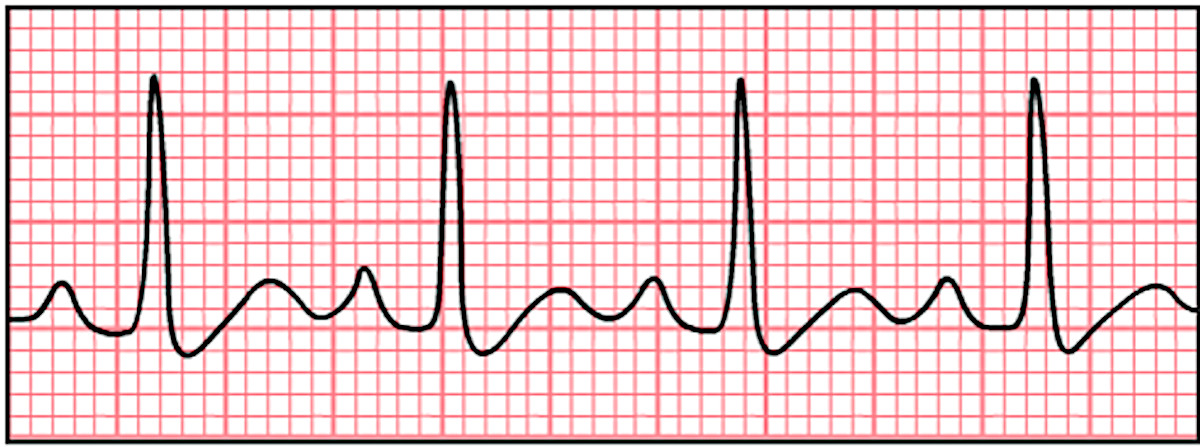
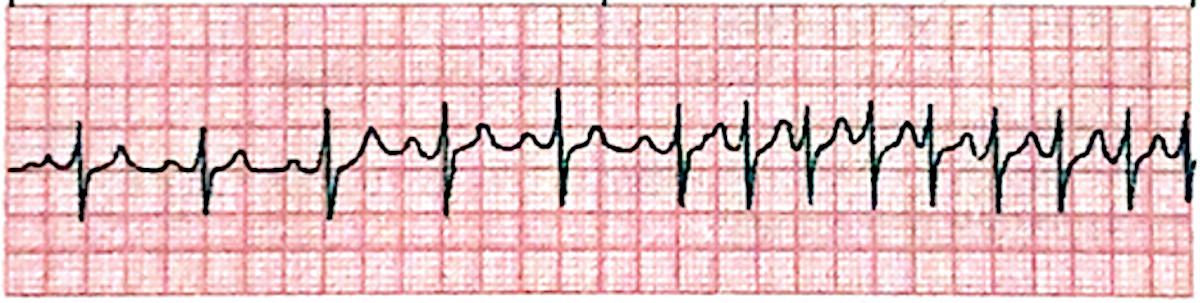
Sinus Tachycardia
Atrial and ventricular rhythms are regular. Rate > 100 bpm. Normal P wave preceding each QRS complex.
Normal physiologic response to fever, exercise, anxiety, dehydration, or pain. May accompany shock, left-sided heart failure, cardiac tamponade, hyperthyroidism, and anemia. Atropine, epinephrine, quinidine, caffeine, nicotine, and alcohol use.
Correction of underlying cause. Beta-adrenergic blockers or calcium channel blockers for symptomatic patients.
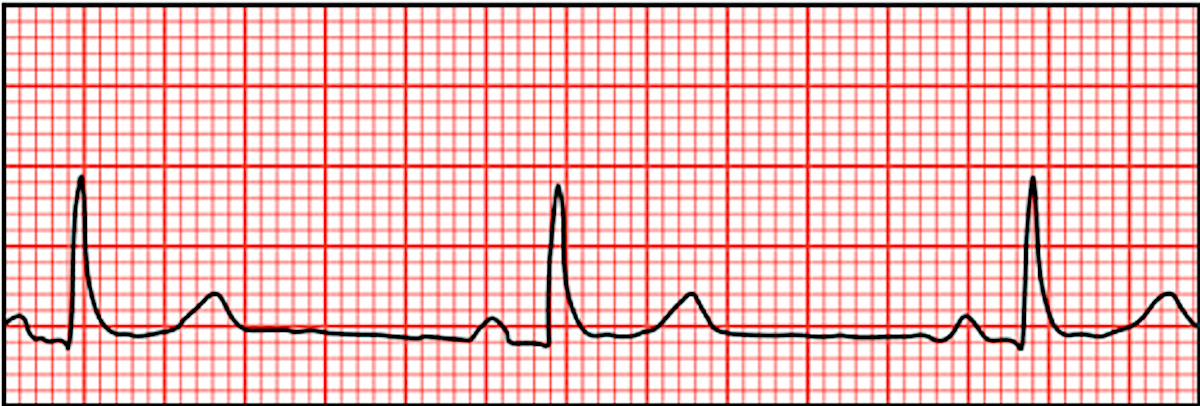
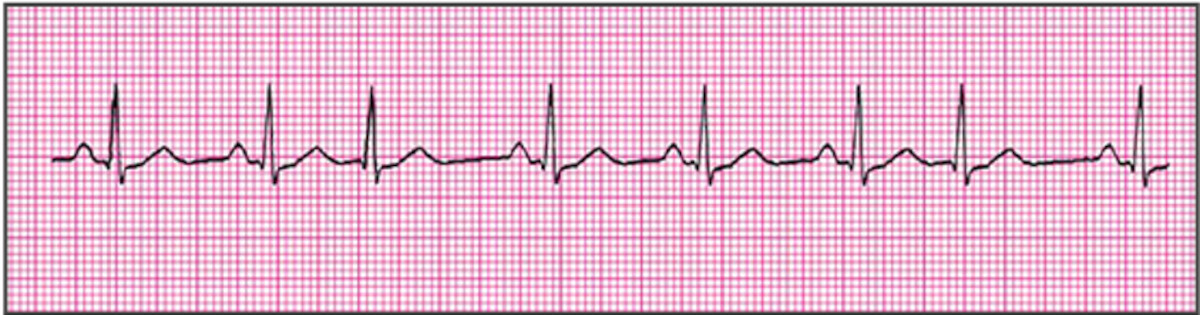
Sinus Bradycardia
Regular atrial and ventricular rhythms. Rate < 60 bpm. Normal P wave preceding each QRS complex.
Normal in a well-conditioned heart (e.g., athletes).
Increased intracranial pressure; increased vagal tone due to straining
during defecation, vomiting, intubation, mechanical ventilation.
Follow ACLS protocol for administration of atropine for symptoms of low
cardiac output, dizziness, weakness, altered LOC, or low blood
pressure. Pacemaker
Sinoatrial (SA) arrest or block
Atrial and ventricular rhythms normal except for missing complex. Normal P wave preceding each QRS complex. Pause not equal to multiple of the previous rhythm.
Treat symptoms with atropine I.V. Temporary pacemaker or permanent pacemaker if considered for repeated episodes.
Wandering atrial pacemaker
Atrial and ventricular rhythms vary slightly. Irregular PR interval.
P waves irregular with changing configurations indicating that they
aren’t all from SA node or single atrial focus; may appear after the QRS
complex. QRS complexes uniform in shape but irregular in rhythm.
Rheumatic carditis due to inflammation involving the SA node. Digoxin toxicity Sick sinus syndrome
No treatment if patient is asymptomatic Treatment of underlying cause if patient is symptomatic.
Premature atrial contraction (PAC)
Premature, abnormal-looking P waves that differ in configuration from normal P waves. QRS complexes after P waves except in very early or blocked PACs. P wave often buried in the preceding T wave or identified in the preceding T wave.
May prelude supraventricular tachycardia. Stimulants, hyperthyroidism, COPD, infection and other heart diseases.
Usually no treatment is needed. Treatment of underlying cause if patient is symptomatic. Carotid sinus massage.
Paroxysmal Supraventricular Tachycardia
Atrial and ventricular rhythms are regular. Heart rate > 160 bpm; rarely exceeds 250 bpm. P waves regular but aberrant; difficult to differentiate from preceding T wave. P wave preceding each QRS complex. Sudden onset and termination of arrhythmia
When a normal P wave is present, it’s called paroxysmal atrial
tachycardia; when a normal P wave isn’t present, it’s called paroxysmal
junctional tachycardia.
Physical exertion, emotion, stimulants, rheumatic heart diseases. Intrinsic abnormality of AV conduction system. Digoxin toxicity. Use of caffeine, marijuana, or central nervous system stimulants.
If patient is unstable prepare for immediate cardioversion. If patient is stable, vagal stimulation, or Valsalva’s maneuver, carotid sinus massage. Adenosine by rapid I.V. bolus injection to rapidly convert arrhythmia. If patient has normal ejection fraction, consider calcium channel blockers, beta-adrenergic blocks or amiodarone. If patient has an ejection fraction less than 40%, consider amiodarone.
Atrial flutter
Atrial rhythm regular, rate, 250 to 400 bpm Ventricular rate variable, depending on degree of AV block Saw-tooth shape P wave configuration. QRS complexes uniform in shape but often irregular in rate.
If patient is unstable with ventricular rate > 150bpm, prepare for immediate cardioversion. If patient is stable, drug therapy may include calcium channel blockers, beta-adrenergic blocks, or antiarrhythmics. Anticoagulation therapy may be necessary.
Atrial Fibrillation
Atrial rhythm grossly irregular rate > 300 to 600 bpm. Ventricular rhythm grossly irregular, rate 160 to 180 bpm. PR interval indiscernible. No P waves, or P waves that appear as erratic, irregular base-line fibrillatory waves
Heart failure, COPD, thyrotoxicosis, constrictive pericarditis,
ischemic heart disease, sepsis, pulmonary embolus, rheumatic heart
disease, hypertension, mitral stenosis, atrial irritation, complication
of coronary bypass or valve replacement surgery
If patient is unstable with ventricular rate > 150bpm, prepare for immediate cardioversion.
If stable, drug therapy may include calcium channel blockers,
beta-adrenergic blockers, digoxin, procainamide, quinidine, ibutilide,
or amiodarone. Anticoagulation therapy to prevent emboli. Dual chamber atrial pacing, implantable atrial pacemaker, or surgical maze procedure may also be used.
Junctional Rhythm
Atrial and ventricular rhythms are regular. Atrial rate 40 to 60 bpm. Ventricular rate usually 40 to 60 bpm. P waves preceding, hidden within (absent), or after QRS complex; usually inverted if visible. PR interval (when present) < 0.12 second QRS complex configuration and duration normal, except in aberrant conduction.
Inferior wall MI, or ischemia, hypoxia, vagal stimulation, sick sinus syndrome. Acute rheumatic fever. Valve surgery Digoxin toxicity
Correction of underlying cause. Atropine for symptomatic slow rate Pacemaker insertion if patient is refractory to drugs Discontinuation of digoxin if appropriate.
Premature Junctional Conjunctions
Atrial and ventricular rhythms are irregular. P waves inverted; may precede be hidden within, or follow QRS complex. QRS complex configuration and duration normal.
MI or ischemia Digoxin toxicity and excessive caffeine or amphetamine use
Correction of underlying cause. Discontinuation of digoxin if appropriate.
First-degree AV block
Atrial and ventricular rhythms regular PR interval > 0.20 second. P wave preceding each QRS complex. QRS complex normal.
Inferior wall MI or ischemia or infarction, hypothyroidism, hypokalemia, hyperkalemia. Digoxin toxicity. Use of quinidine, procainamide, beta-adrenergic blockers, calcium
Correction of the underlying cause. Possibly atropine if PR interval exceeds 0.26 second or symptomatic bradycardia develops. Cautious use of digoxin, calcium channel blockers, and beta-adrenergic blockers.
Second-degree AV block Mobitz I (Wenckebach)
Atrial rhythm regular. Ventricular rhythm irregular. Atrial rate exceeds ventricular rate. PR interval progressively, but only slightly, longer with each cycle until QRS complex disappears. PR interval shorter after dropped beat.
Atropine, epinephrine, and dopamine for symptomatic bradycardia. Temporary or permanent pacemaker for symptomatic bradycardia. Discontinuation of digoxin if appropriate.
Third-degree AV block (complex heart block)
Atrial rhythm regular. Ventricular rhythm regular and rate slower than atrial rate. No relation between P waves and QRS complexes. No constant PR interval. QRS interval normal (nodal pacemaker) or wide and bizarre (ventricular pacemaker).
Inferior or anterior wall MI, congenital abnormality, rheumatic fever.
Atropine, epinephrine, and dopamine for symptomatic bradycardia. Temporary or permanent pacemaker for symptomatic bradycardia.
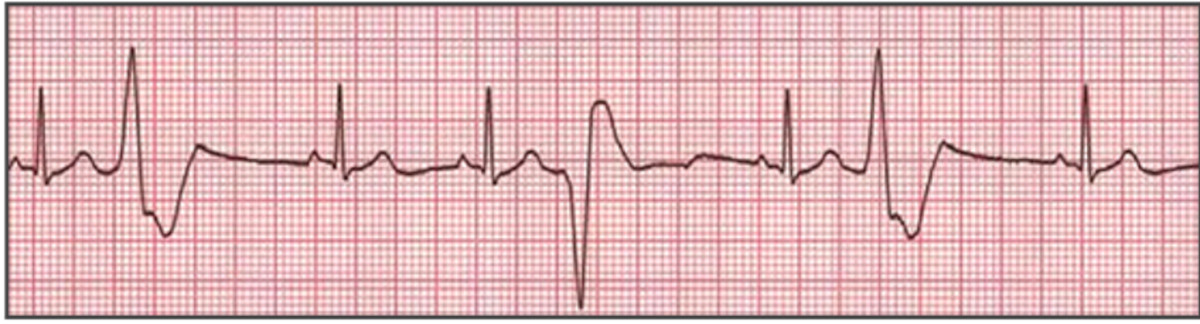
Premature ventricular contraction (PVC)
Atrial rhythm regular Ventricular rhythm irregular QRS complex premature, usually followed by a complete compensatory pause QRS complex wide and distorted, usually >0.14 second.
Premature QRS complexes occurring singly, in pairs, or in threes;
alternating with normal beats; focus from one or more sites. Ominous when clustered, multifocal, with R wave on T pattern.
Heart failure; old or acute myocardial ischemia, infarction, or contusion. Myocardial irritation by ventricular catheters such as a pacemaker. Hypercapnia, hypokalemia, hypocalcemia. Drug toxicity by cardiac glycosides, aminophylline, tricyclic antidepressants, beta-adrenergic. Caffeine, tobacco, or alcohol use. Psychological stress, anxiety, pain
If warranted, procainamide, lidocaine, or amiodarone I.V. Treatment of underlying cause. Discontinuation of drug causing toxicity. Potassium chloride IV if PVC induced by hypokalemia. Magnesium sulfate IV if PVC induced by hypomagnesaemia.
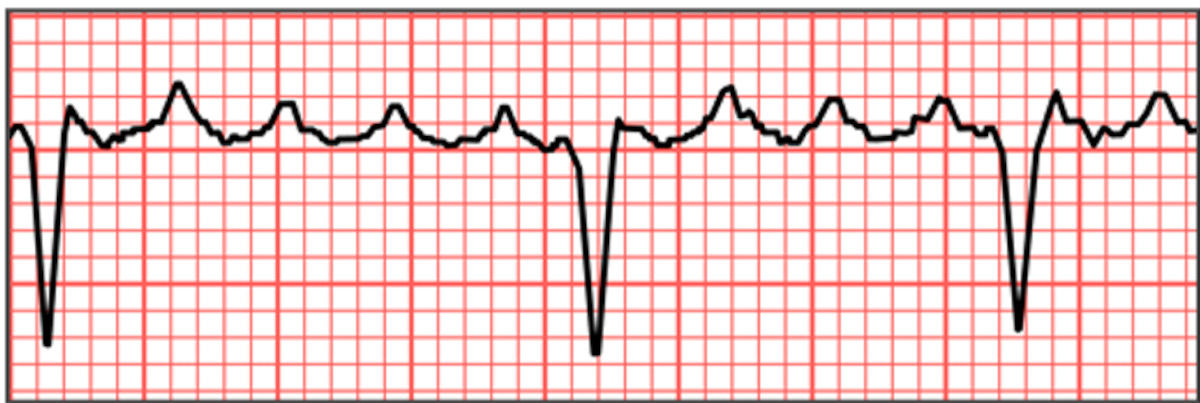
Ventricular Tachycardia
Ventricular rate 140 to 220 bpm, regular or irregular. QRS complexes wide, bizarre, and independent of P waves P waves no discernible May start and stop suddenly
If pulseless: initiate CPR; follow ACLS protocol for defibrillation.
If with pulse: If hemodynamically stable, follow ACLS protocol for
administration of amiodarone; if ineffective initiate synchronized
cardioversion.
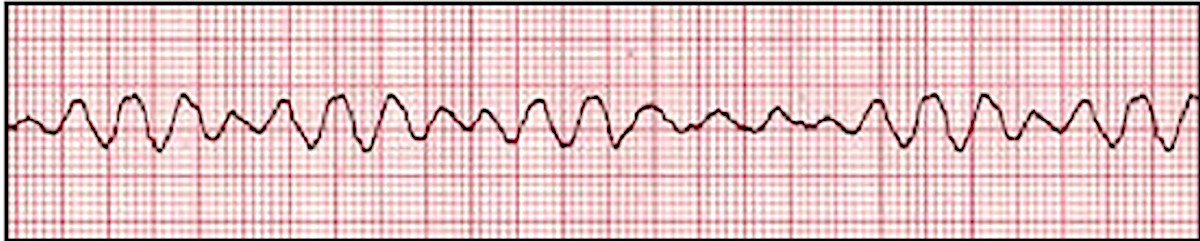
Ventricular Fibrillation
Ventricular rhythm and rate are rapid and chaotic. QRS complexes wide and irregular, no visible P waves
Myocardial ischemia or infarction, R-on-T phenomenon, untreated ventricular tachycardia, Hypokalemia, hyperkalemia, Hypercalcemia, alkalosis, electric shock, hypothermia. Digoxin, epinephrine, or quinidine toxicity.
If pulseless: start CPR, follow ACLS protocol for defibrillation, ET
intubation, and administration f epinephrine or vasopressin, lidocaine,
or amiodarone; ineffective consider magnesium sulfate.
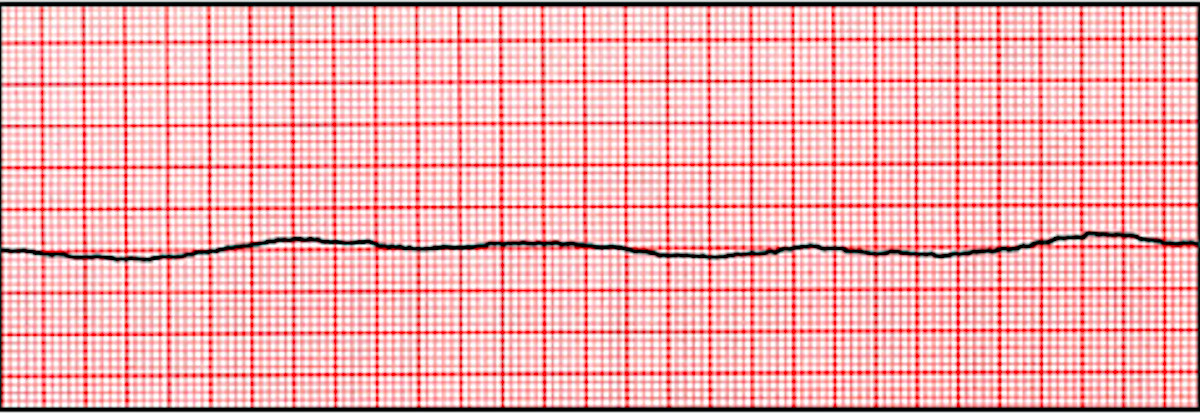
Asystole
No atrial or ventricular rate or rhythm. No discernible P waves, QRS complexes, or T waves
Myocardial ischemia or infarction, aortic valve disease, heart failure,
hypoxemia, hypokalemia, severe acidosis, electric shock, ventricular
arrhythmias, AV block, pulmonary embolism, heart rupture, cardiac
tamponade, hyperkalemia, electromechanical dissociation. Cocaine overdose.